A 503B Outsourcing Facility is a designation that was created by Congress in the Drug Quality & Security Act to bridge the gap between traditional state-licensed compounding pharmacies and industrial pharmaceutical manufacturers. 503B Outsourcing Facilities must register with FDA and adhere to cGMP (Current Good Manufacturing Practices) standards. 503B Outsourcing Facilities provide access to compounded medications for office use, enabling you to begin treatment as soon as possible.
Offering the combined formularies of both a traditional state-licensed compounding pharmacy and 503B Outsourcing Facility allows us to provide a full spectrum of high-quality medications, ranging from highly customized compounded medications for patient-specific prescriptions to office-use items you always need on your shelf.
You can continue to access our entire formulary, including those prepared at Wedgewood Connect, through our Customer Care team at 800-216-5005, or simply fax this form to 800-589-4250.
We are dedicated to continuous innovation and look forward to expanding our 503B formulary to include more of the medications your practice and patients rely on.

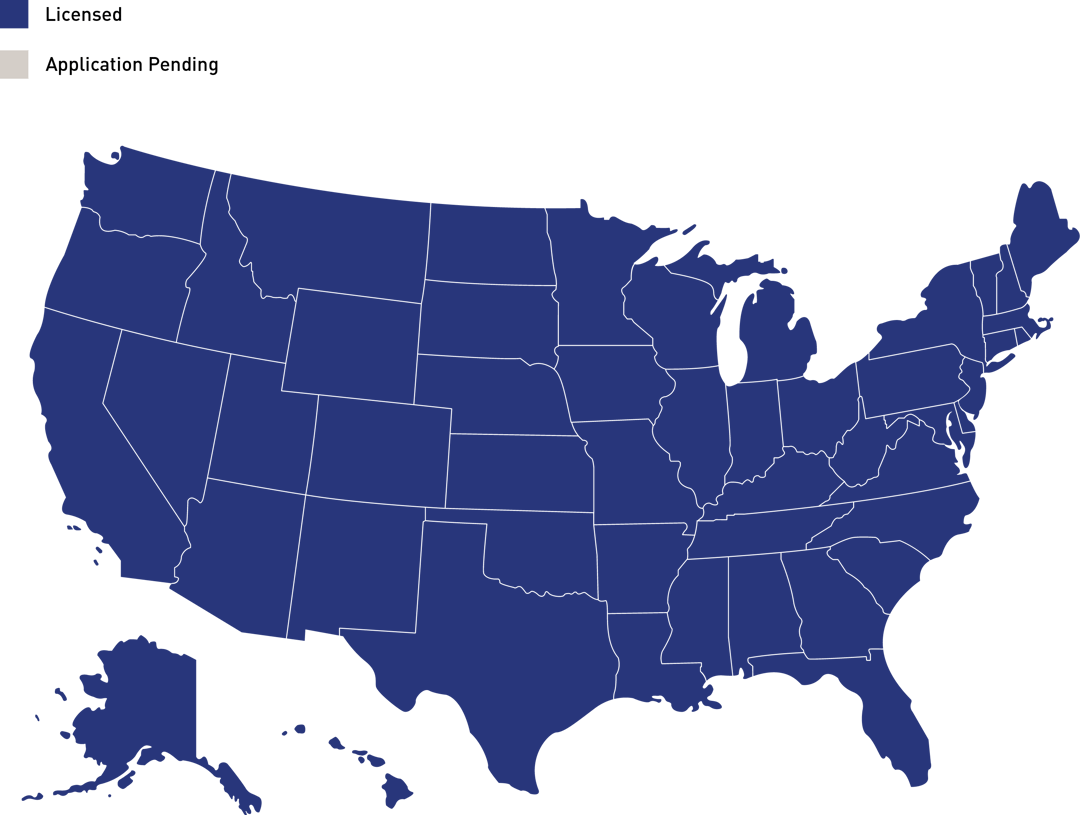
Wedgewood Connect is currently licensed as a 503B Outsourcing Facility in all 50 states. Medications prepared at Wedgewood Connect can be ordered for office use in all states except HI. Medications prepared at Wedgewood Connect can be prescribed in all states except SC.